Vasculitis is defined as inflammation of blood vessels, affecting their structure and function, and resulting in weakening, narrowing, and scarring of the vessel wall. Vasculitis presentations are categorized based on the size, type, and location of the affected vessels.1 Leukocytoclastic vasculitis (LCV) is categorized as ‘small vessel vasculitis’, where the inflammatory infiltrate is composed of neutrophils.2 Cutaneous LCV tends to present as palpable purpura in the skin of the lower limbs.1
Drugs are among the most common triggers of LCV, and the signs and symptoms typically begin to manifest around 1–3 weeks after the initiation of the drug. Beta-lactams, vancomycin, erythromycin, clindamycin, sulfonamides, allopurinol, nonsteroidal anti-Inflammatory drugs, furosemide, thiazides, beta-blockers, gold, phenytoin, valproic acid, metformin, warfarin, and selective serotonin reuptake inhibitors are among the common causes of LCV.3 Early withdrawal of the offending drug is usually sufficient for rapid resolution and recovery.4
Tigecycline-induced LCV is rare. One case was reported in 2015, with a sudden skin eruption of macular purpuric rash symmetrically distributed on lower limbs.5 Here we present a case of tigecycline induced LCV with an atypical clinical presentation.
Case Report
Our patient was a 44-year-old Omani man with a history of uncontrolled hypertension and uncontrolled type 2 diabetes with end-stage renal disease on regular hemodialysis. He had undergone left lower limb above-knee amputation. He also suffered from hepatitis C, ascites, and ischemic heart disease with an ejection fraction 30–50%. Additionally, he had recurrent bilateral pleural effusion that required multiple pleural taps.
The patient presented with right-sided pleural effusion complicated by a parapneumonic effusion, along with fever and elevated inflammatory markers. He was admitted and started on intravenous Tazocin® (a combination of piperacillin and tazobactam). He underwent a right posterolateral thoracotomy for decortication and drainage of the pleural effusion and was maintained on epidural analgesia for pain control. He had persistent leukocytosis and elevated inflammatory markers, so the infectious disease team stopped Tazocin and started him on tigecycline until the final sensitivity results of his screening samples were available.
Three days after starting tigecycline, the patient developed a sudden, asymptomatic, progressive erythematous skin eruptions symmetrically distributed on the upper extremities and ears. There were multiple grouped purpuric papulovesicular lesions coalescing to form plaques on erythematous background distributed symmetrically over the upper extremities and lateral surface of both ears. The palms were spared. Oral examination revealed purpuric maculopapular lesions on the hard palate and healed ulcers on the left buccal mucosa. The face, trunk, lower extremities, and genital area were not affected [Figure 1]. The patient was conscious, alert, afebrile, and had normal vital signs. Dermatoscopy showed hemorrhagic blisters, purpuric globules, and dots on orange-brown background [Figure 2].
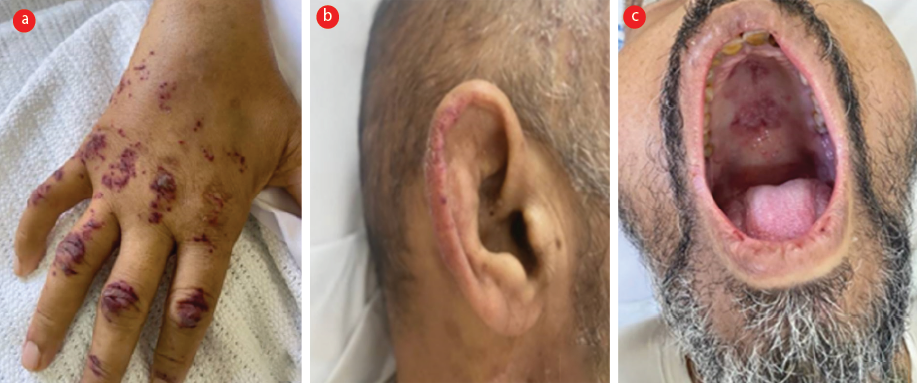 Figure 1: (a) Grouped hemorrhagic blisters with purpuric background in dorsum of right hand. (b) Purpuric macules over the helix of right ear. (c) Grouped hemorrhagic blisters in the hard palate.
Figure 1: (a) Grouped hemorrhagic blisters with purpuric background in dorsum of right hand. (b) Purpuric macules over the helix of right ear. (c) Grouped hemorrhagic blisters in the hard palate.
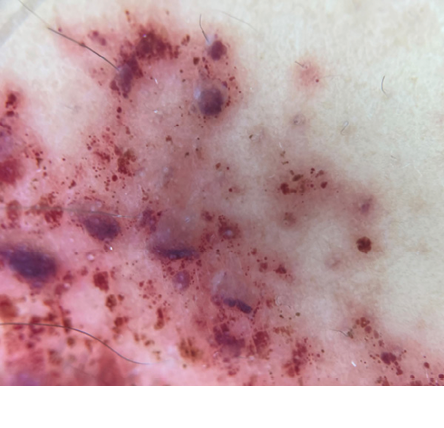 Figure 2: Dermatoscopy image showing hemorrhagic blisters and purpuric globules and dots on orange-brown background.
Figure 2: Dermatoscopy image showing hemorrhagic blisters and purpuric globules and dots on orange-brown background.
The clinical impression was that of leukocytoclastic vasculitis, likely induced by the new antibiotic tigecycline, which was immediately replaced with meropenem. As herpes zoster infection with multi-dermatomal involvement was also considered a possibility, vesicular fluid was sent for polymerase chain reaction testing for varicella-zoster virus (VZV PCR). While awaiting results, the antiviral acyclovir was started intravenously.
Laboratory results revealed low hemoglobin (8.9 g/dL), mild neutrophilia (5.2 109/L), a normal platelet count, and raised C-reactive protein (167 mg/L). Derangement of coagulation profile yielded prothrombin time of 17.5 sec, activated partial thromboplastin time of 53.6 sec, thrombin time of 25.8 sec, and international normalized ratio of 1.72. Renal function test yielded estimated glomerular filtration rate of 18 mL/min/1.73 m2, creatinine of 325 umol/L, and potassium ion of 5.3 mmol/L. Liver function results were normal except for raised alkaline phosphatase (176 U/L) and hypoalbuminemia (22 g/L). When the results for herpes simplex virus and VZV PCR came negative, acyclovir intravenously was discontinued.
Two skin punch biopsies from right forearm were sent for histopathology and immunofluorescence studies. Immunofluorescence result was negative. Histopathological examination revealed clefting at the dermoepidermal junction, and the underlying dermis showed perivascular inflammation [Figure 3]. At higher magnification, neutrophils were visible in the wall of blood vessels with fibrinoid necrosis [Figure 4]. Neutrophilic nuclear dust was also seen in the dermis. These features are typical for LCV. Thus skin punch biopsy confirmed the diagnosis of LCV as suspected.
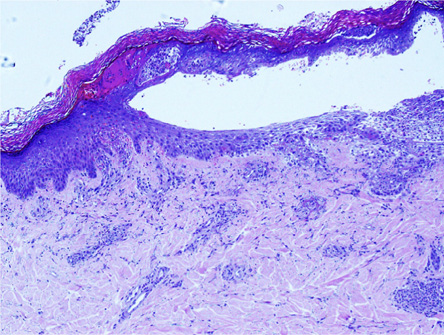 Figure 3: Hematoxylin-eosin stained shows cleft at dermo epidermal junction with perivascular inflammation, magnification = 4 ×.
Figure 3: Hematoxylin-eosin stained shows cleft at dermo epidermal junction with perivascular inflammation, magnification = 4 ×.
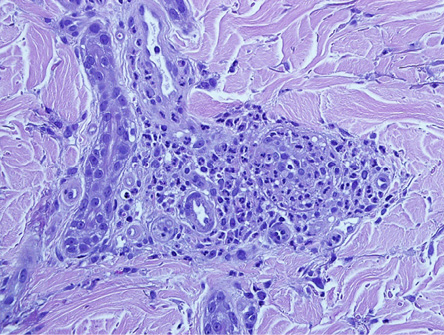 Figure 4: Hematoxylin-eosin stained shows neutrophils in the wall of blood vessel with fibrinoid necrosis, magnification = 20 ×.
Figure 4: Hematoxylin-eosin stained shows neutrophils in the wall of blood vessel with fibrinoid necrosis, magnification = 20 ×.
After three days of stopping tigecycline, some vesicles deroofed and there were crusted lesions over right and left hand. The rash became duskier in color, and the lesions over the left ear became crusted. The patient was discharged after 10 days in stable condition, with dramatic improvement in his skin condition.
Discussion
About 10% of LCV cases are drug induced. Some recent cases were associated with COVID-19 vaccination.6,7 Tigecycline belongs to the newer class of powerful tetracycline-derived antibiotics and has an extraordinarily broad spectrum of activity against many resistant gram-positive, gram-negative, and anaerobic pathogens.8 On the downside, tetracycline derivatives have been reported to induce autoimmunity conditions such as anti-nuclear cytoplasmic antibody (ANCA)-associated vasculitis, cutaneous polyarteritis nodosa, and drug induced lupus.9
In our patient, there was clear evidence that tigecycline caused LCV, because the cutaneous lesions improved within three days of discontinuating the drug without the need for systemic therapy. We found only one case in the literature reported as tigecycline-induced LCV.5 Thus our case is the second one. Additionally, to our knowledge, this is the first reported case reporting tigecycline-induced hemorrhagic vesiculobullous LCV on the upper extremities.
Leukocytoclastic vasculitis is caused by activation of the complement system and deposition of immune complex is walls of small blood vessels. After the recruitment of neutrophils, subsequent exudation of erythrocytes, fibrin, and serum occurs along with damage to the vessel walls. The small vessel walls will exhibit fibrinous necrosis as a result of lysosomal enzymes like collagenases and elastases as well as reactive oxygen species. The development of clinical findings is also aided by lymphokines. Increased levels of interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor may be found in the blood. The lower extremities’ turbulence and elevated venous pressure may help explain why LCV frequently affects the leg.10
In our patient, however, the rash started on the upper extremities and ears sparing the trunk and lower extremities, which is unusual for the cutaneous vasculitis. His skin eruptions were asymptomatic, probably because he was on strong analgesia. The grouped hemorrhagic vesiculobullous lesions resembled those seen in multidermatomal herpes zoster infection in immune compromised patients, especially the lesions on hard palate. This initially caused diagnostic uncertainty, particularly because HCV is known to be associated with the pathogenesis of LCV.11 The negative herpes simplex virus and VZV PCR results ruled out that possibility. The unusual presentation of LCV in our patient might be attributable to his complex medical history including peripheral vasculopathy secondary to ischemic heart disease and uncontrolled hypertension and diabetes that necessitated a limb amputation.
If LCV is suspected, a skin punch biopsy should be performed along with direct immunofluorescence studies. It is recommended to choose a site with blue-gray blotch, which is considered the most specific dermoscopic feature for true vasculitis.12 Essential laboratory tests include complete blood counts, renal function and liver function tests, and urinalysis, with more extensive work-up in case of systemic involvement.13
Diagnosing drug-induced LCV might be challenging. However, recognizing the clinical features and resolution of cutaneous manifestations after discontinuation of the offending drug can aid in the diagnosis.2 As in the current case, cutaneous LCV has an excellent prognosis if it is limited to the skin and diagnosed early.
Conclusion
LCV is an extremely rare side-effect of the new-generation antibiotic tigecycline, the present case being the second one to be reported. Drug-induced LCV should be suspected when a patient develops new skin eruptions following recently started medication. Skin biopsy for routine histological and immunofluorescence studies remains the diagnostic gold standard for LCV. It should also be kept in mind that cutaneous vasculitis does not necessarily begin on the lower extremities.
Disclosure
The authors declare no conflicts of interest. Written consent of the patient was obtained to publish this case report.
references
- 1. Younger DS, Carlson A. Dermatologic aspects of systemic vasculitis. Neurol Clin 2019 May;37(2):465-473.
- 2. Kossard S. Defining lymphocytic vasculitis. Australas J Dermatol 2000 Aug;41(3):149-155.
- 3. Fekete GL, Fekete L. Cutaneous leukocytoclastic vasculitis associated with erlotinib treatment: a case report and review of the literature. Exp Ther Med 2019 Feb;17(2):1128-1131.
- 4. Lee HL, Kim L, Kim CW, Kim JS, Nam HS, Ryu JS. Case of both rivaroxaban- and dabigatran-induced leukocytoclastic vasculitis, during management of pulmonary thromboembolism. Respir Med Case Rep 2019 Jan;26:219-222.
- 5. Bhairavarasu K, Mocherla S, Amaram J, Sharma E, Colin PA, Umer I. Drug-induced leukocytoclastic vasculitis: tigecycline a rare cause. The Southwest Respiratory and Critical Care Chronicles 2015;3(9):55-58.
- 6. Fiorillo G, Pancetti S, Cortese A, Toso F, Manara S, Costanzo A, et al. Leukocytoclastic vasculitis (cutaneous small-vessel vasculitis) after COVID-19 vaccination. J Autoimmun 2022 Feb;127:102783.
- 7. Ball-Burack MR, Kosowsky JM. A case of leukocytoclastic vasculitis following SARS-COV-2 vaccination. J Emerg Med 2022 Aug;63(2):e62-e65.
- 8. Slover CM, Rodvold KA, Danziger LH. Tigecycline: a novel broad spectrum antimicrobial. Ann Pharmacother 2007 Jun;41(6):965-672.
- 9. Alquorain NA, Aljabr AS, Alghamdi NJ. Cutaneous polyarteritis nodosa treated with pentoxifylline and clobetasol propionate: a case report. Saudi J Med Med Sci 2018;6(2):104-107.
- 10. Shavit E, Alavi A, Sibbald RG. Vasculitis-what do we have to know? A review of literature. Int J Low Extrem Wounds 2018 Dec;17(4):218-226.
- 11. Bernacchi E, Civita LL, Caproni M, Zignego AL, Bianchi B, Monti M, et al. Hepatitis C virus (HCV) in cryoglobulinaemic leukocytoclastic vasculitis (LCV): could the presence of HCV in skin lesions be related to T CD8+ lymphocytes, HLA-DR and ICAM-1 expression? Exp Dermatol 1999 Dec;8(6):480-486.
- 12. Choo JY, Bae JM, Lee JH, Lee JY, Park YM. Blue-gray blotch: a helpful dermoscopic finding in optimal biopsy site selection for true vasculitis. J Am Acad Dermatol 2016 Oct;75(4):836-838.
- 13. Carlson JA, Ng BT, Chen KR. Cutaneous vasculitis update: diagnostic criteria, classification, epidemiology, etiology, pathogenesis, evaluation and prognosis. Am J Dermatopathol 2005 Dec;27(6):504-528.