Multiple sclerosis (MS) is an autoimmune disease of the central nervous system (CNS) and the most prevalent chronic inflammatory CNS disorder, impacting 2.5 million people globally.1 The clinical phenotypes of MS are not distinguishable from one another. Therefore, MS can only be diagnosed with a combination of physical findings, laboratory assays, and imaging, especially magnetic resonance imaging.2 MS has a complex etiology and can present with a wide variety of symptoms, the most reported ones being ataxia, cognitive impairment, and visual loss.2
There are four major forms of MS. Clinically isolated syndrome (CIS) describes the first clinical onset of potential MS. More definite and chronic forms include relapsing-remitting MS (RRMS), primary progressive MS (PPMS), and secondary progressive MS (SPMS). RRMS, which represents the majority (~ 85%) of MS cases, follows a chronic repetitive pattern of relapses and remissions.3 Most patients with RRMS eventually transition to SPMS, characterized by gradual worsening of disability over time.3 SPMS initially follows an RRMS course, and thereafter gradually worsens over time.4 PPMS patients’ symptoms worsen over time and never improve.
While the etiology of MS is not fully understood, growing evidence implicates neurodegeneration that arises from inflammatory demyelination, triggered by peripheral immune activation.5 Early in the disease, inflammatory lymphocytes, macrophages, and activated microglia infiltrate the affected area in the CNS. This leads to an overproduction of inflammatory mediators, causing demyelination and axonal conduction block, ultimately resulting in the neurological disabilities typical of MS.6,7
This sterile inflammation (not triggered by pathogens) is driven by innate inflammatory inducers during tissue damage.5 The resulting stress-associated molecular patterns are detected by inflammasomes, initiating downstream inflammatory signaling.7
Inflammasomes are multi-protein complexes in the cytosol with three main components: an upstream sensor nucleotide-binding oligomerization domain-like receptor (NLR) protein, a middle protein called an apoptosis-associated speck-like protein containing a CARD, and a downstream effector protein, caspase-1.8 On being stimulated by microbial or damage-associated molecular patterns, the NLRs assemble into an inflammatory complex that triggers the autocatalytic cleavage of caspase-1, transforming proinflammatory cytokines interleukin-1 beta (IL-1β) and IL-18 into their biologically active forms.8 Many studies have implicated dysregulated activation of inflammasome and the increased expression of caspase-1, IL-1β, and IL-18 for contributing to the development and progression of autoimmune diseases.9
Oxidative stress arises when the production of reactive oxygen species (ROS) exceeds the capacity of the cellular detoxification systems. This imbalance can prime and activate the inflammasome pathway.10 The ROS generated in brain tissue can modulate both synaptic and non-synaptic neuroinflammatory communications, contributing to neurodegeneration and loss of memory.11 Multiple activators of NLRP3 increase mitochondrial ROS generation, whereas preincubation with antioxidants suppresses inflammatory pathways dependent on NLRP3.12 Antioxidants such as vitamins D and E play a crucial role in neutralizing free radicals that cause cellular damage.13 The significance of these vitamins in the pathophysiology of MS has been investigated in depth.14,15
Conversely, increased generation of inflammatory markers can deplete antioxidant vitamin levels.16 The individual effects of vitamins D and E on the NLRP3 inflammasome pathway in MS have been described. Vitamin D levels suppress NLRP3 inflammasome activation and downstream IL-1β signaling.17,18 Vitamin E analogues suppress NLRP3 inflammasome and protect against inflammation.19
However, to our knowledge, no prior studies have evaluated the combined influence of vitamins D and E on the inflammasome markers IL-18, IL-1β, and NLRP3 in MS. To address this gap in literature, we aimed to determine the association between IL-18, IL-1β, and NLRP3 levels and antioxidant vitamins D and E in patients with MS.
Methods
The study was approved by the institutional review boards at King Abdullah University Hospital, Irbid, Jordan (Ref. 162/132/2020), and Al-Bashir Hospital, Amman, Jordan (Ref. 4718, 21/3/2022). Written informed consent was obtained from all subjects before participation.
The study included adults aged 18–70 years with a neurologist-confirmed diagnosis of MS according to the revised McDonald criteria,20 and the ability to provide written informed consent. Patients with chronic diseases other than MS (e.g., diabetes mellitus, kidney diseases, or cardiovascular disease) were excluded.
Participants were recruited through convenience sampling from private and public neurology clinics in Jordan. A total of 100 patients with MS were enrolled and divided into two groups based on MS subtype: RRMS (n = 30); PP/SP MS (n = 70). The control group comprised 100 apparently healthy volunteers from Jordan University of Science and Technology, matched to MS group in age, sex, and body mass index.
For each participant, 10 mL venous blood was collected in a plain tube without a clot activator. Samples were centrifuged at 3000 × g for 10 minutes to separate the serum, which was frozen at -80 °C until analysis. All serum samples were subjected to enzyme-linked immunosorbent assay to determine the levels of NLRP3 (MyBioSource, USA), IL-1β, IL-18 (R&D Systems, USA), and vitamin E and vitamin D (MyBioSource, USA). Absorbance was read at 450 nm using an ELx800 Microplate Reader (BioTek Instruments, USA). Manufacturers’ instructions were strictly followed.
Statistical analyses were performed with GraphPad Prism 9 (GraphPad Software, San Diego, CA). Student t-test was used to compare serum levels of inflammasome markers and vitamins between MS and control groups and between RRMS and PP/SP MS subgroups. Pearson’s correlation coefficient (r) assessed the correlations between vitamin levels and inflammasome markers. Data were reported as mean ± standard error of mean. A p-value < 0.05 was considered statistically significant.
Results
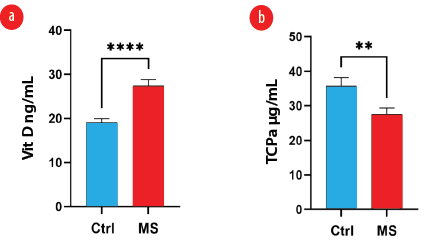
A total of 200 participants—100 patients with MS and 100 matched controls—were enrolled in the study. Serum levels of NLRP3, IL-1β, and IL-18 were significantly elevated in the MS group compared with the control group (p = 0.040, p < 0.001, and p = 0.020, respectively) [Table 1, Figure 1]. Vitamin D levels were significantly higher (p < 0.01) and vitamin E significantly lower in MS patients compared to control (p = 0.006) [Table 1, Figure 2].
Table 1: Clinical and demographic data of multiple sclerosis patients and healthy controls (N = 200).
|
Age, years
|
36.5
|
1.0
|
34.7
|
0.2
|
0.100
|
|
Sex
|
|
|
|
|
0.880
|
|
Female
|
68
|
-
|
67
|
-
|
|
|
Male
|
32
|
-
|
33
|
-
|
|
|
BMI, kg/m2
|
27.5
|
1.8
|
27.9
|
0.3
|
0.830
|
|
IL-18, pg/mL
|
229.2
|
10.9
|
197.3
|
9.1
|
0.020*
|
|
Vitamin D, ng/mL
|
27.5
|
1.3
|
19.0
|
0.8
|
< 0.010*
|
|
Vitamin E, µg/mL
|
27.6
|
1.7
|
35.8
|
2.4
|
0.006*
|
|
NLRP3, pg/mL
|
150.1
|
5.7
|
133.3
|
6.0
|
0.040*
|
SEM: standard error of mean; BMI: body mass index; IL-18: interleukin-18; NLRP3: nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3; IL-1β: interleukin-1 beta. *Significant.

MS: multiple sclerosis; Ctrl: controls; NLRP3: nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3; IL-1β: interleukin-1 beta; IL-18: interleukin-18.
Figure 1: Comparative levels of inflammasome markers in MS patients (n = 100) and controls (n = 100). (a) NLRP3 (p < 0.050), (b) IL-1β (p < 0.001), (c) IL-18 (p < 0.050).
MS: multiple sclerosis; Ctrl: controls; TCPa: alpha-tocopherol.
Figure 2: Comparative antioxidant vitamin serum levels in MS patients (n = 100) and controls (n = 100). (a) Vitamin D (p < 0.010); (b) vitamin E (TCPa)
(p = 0.006).
NLRP3, IL-1β, IL-18, vitamin D, and vitamin E levels were not significantly different between patients with RRMS and PP/SP MS [Table 2].
Table 2: Comparative data of patients with RRMS and PP/SP MS.
|
Age, years
|
37.5 ± 1.8
|
35.9 ± 1.3
|
0.500
|
|
Sex
|
|
|
0.780
|
|
Female
|
21
|
47
|
|
Male
|
9
|
23
|
|
BMI, kg/m2
|
25.4 ± 0.9
|
28.6 ± 2.8
|
0.420
|
|
IL-18, pg/mL
|
232.2 ± 22.6
|
227.9 ± 12.3
|
0.860
|
|
Vitamin D, ng/mL
|
24.8 ± 2.8
|
28.53 ± 1.5
|
0.220
|
|
Vitamin E, µg/mL
|
29.6 ± 3.7
|
26.78 ± 1.8
|
0.460
|
|
NLRP3, pg/mL
|
142.9 ± 9.0
|
152.8 ± 7.1
|
0.420
|
SEM: standard error of mean; RRMS: relapsing-remitting multiple sclerosis; PP: primary progressive; SP: secondary progressive; BMI: body mass index; IL-18: interleukin-18; NLRP3: nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3; IL-1β: interleukin-1 beta.
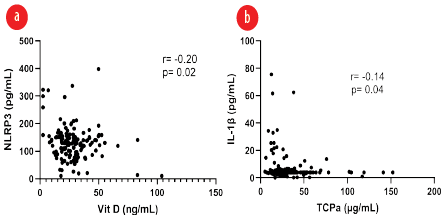
Table 3 describes the correlations between levels of vitamin D and E and inflammasome markers (IL-18, NLRP3, and IL-1β). NLRP3 had a significant weak inverse correlation with vitamin D (r = -0.20, p = 0.020). IL-1β had a significant weak inverse correlation with vitamin E levels (r = -0.14, p = 0.040). IL-18 was not associated with either vitamin [Table 3, Figure 3].
Table 3: Correlation between serum levels of vitamin D and vitamin E with inflammasome markers (IL-18, NLRP3, and IL-1β).
|
IL-18
|
0.07
|
0.310
|
-0.03
|
0.640
|
|
NLRP3
|
-0.20
|
0.020*
|
-0.03
|
0.710
|
r: Pearson rank correlation coefficient; IL-18: Interleukin-18; NLRP3: Nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3; IL-1β: Interleukin-1 beta. *p < 0.05: Significant.
MS: multiple sclerosis.
Figure 3: Pearson correlation coefficient comparisons showing significant negative associations. (a) Serum vitamin D vs. NLRP3
(p = 0.020). (b) Serum vitamin E (TCPa) vs. IL-1β (p = 0.040).
Table 4 shows the results of multiple linear regression analysis, which found no significant associations between age, sex, body mass index and the serum levels of vitamin D, vitamin E, NLRP3, IL-1β for patients with MS.
Table 4: Multiple linear regression model of covariates (age, sex, and BMI) with serum vitamin D, vitamin E, NLRP3, or IL-1β as dependent variables in patients with MS.
|
Age
|
-0.007
|
-0.107
|
0.915
|
0.055
|
0.798
|
0.426
|
-0.013
|
-0.189
|
0.851
|
0.012
|
0.179
|
0.858
|
|
BMI
|
-0.051
|
-0.736
|
0.462
|
0.040
|
0.578
|
0.564
|
0.014
|
0.198
|
0.843
|
0.125
|
1.821
|
0.070
|
BMI: body mass index; NLRP3: nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3; IL-1β: interleukin-1 beta.
Discussion
The link between inflammasome activation and the combined levels of antioxidant vitamins D and E in MS have been underexplored. This study has demonstrated existence of significant associations between vitamins D and E and inflammasome markers (IL-18, NLRP3, and IL-1β) in Jordanian patients with MS.
Serum levels of IL-18, NLRP3, and IL-1β were significantly higher in MS patients than in healthy controls, consistent with findings from an Iranian study.21 The NLRP3 inflammasome can be activated by a broad range of stimuli, both microbial and sterile.22 The consequent release of the proinflammatory cytokines IL 1β and IL 18 is considered to contribute to the pathogenesis of MS.23 In a mouse model, knocking out the NLRP3 gene (NLRP3-/-) significantly delayed the onset of MS and reduced disease severity.24
Vitamin D levels were higher in patients with MS than in the control group, possibly because patients were taking supplements.25 However, both groups had lower-than-recommended levels of vitamin D, as previously reported in Jordanian population.26,27 Vitamin E levels were lower in patients with MS than in the control group, similar to a study in Italy.28 Myelin breakdown and axonal degeneration are two hallmarks of MS pathogenesis, and inflammation that characterizes the condition may be influenced by heightened oxidative stress.29 Vitamin E, a nonenzymatic antioxidant, may become depleted while neutralizing increased number of free radicals during oxidative stress and inflammation.30
In our study, vitamin D showed a weak inverse correlation with NLRP3, while vitamin E inversely correlated with IL-1β. Both vitamins are known to suppress the production of proinflammatory cytokines and inhibit the activation of the NLRP3 inflammasome in macrophages.10,31,32 Several studies have linked insufficient vitamin D levels to increased expression of inflammasome markers.33
Taken together, our findings (inverse correlations between inflammatory markers and antioxidant vitamin levels) suggest that MS cases could be better managed by modulating inflammasome activity. Previous work has shown that interferon-beta, a standard MS therapy, lowers the expression of absent in melanoma 2, an inflammasome sensor linked to IL-1β production.34 Furthermore, antioxidant analogues such as vitamin E may reduce inflammatory cytokine production and block inflammasome activation.19
This study has limitations. The convenience sampling method we used may have introduced a selection bias. Second, MS patients’ medications and supplements may have influenced their serum marker levels. Third, levels of some relevant antioxidants such as caspase-1 and vitamins A and C were not measured. Despite limitations, this is the first study to correlate inflammasome biomarkers with two antioxidant vitamins in patients with MS.
Conclusion
This pioneering study demonstrates an association between inflammasome activity and reduced vitamin levels in MS. Specifically, NLRP3 and IL-1β showed inverse correlations with the nonenzymatic antioxidants (vitamin D and E), respectively, showing the inverse association between inflammasome activation and antioxidant vitamin levels in MS. Our findings may aid in a better understanding of the disease’s complex pathogenic pathways and facilitate better management of vitamin levels, which may help in the discovery of potential diagnostic, prognostic, and therapeutic biomarkers for MS. Further studies are recommended to confirm our findings and to clarify inflammasome’s role and its link with antioxidant vitamins in MS.
Disclosure
The authors declare no conflicts of interest. No funding was received for this study.
references
- 1. Voet S, Prinz M, van Loo G. Microglia in central nervous system inflammation and multiple sclerosis pathology. Trends Mol Med 2019 Feb;25(2):112-123.
- 2. Filippi M, Preziosa P, Arnold DL, Barkhof F, Harrison DM, Maggi P, et al. Present and future of the diagnostic work-up of multiple sclerosis: the imaging perspective. J Neurol 2023 Mar;270(3):1286-1299.
- 3. Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sørensen PS, Thompson AJ, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology 2014 Jul;83(3):278-286.
- 4. Martynova E, Khaibullin T, Salafutdinov I, Markelova M, Laikov A, Lopukhov L, et al. Seasonal changes in serum metabolites in multiple sclerosis relapse. Int J Mol Sci 2023 Feb;24(4):3542.
- 5. Vidmar L, Maver A, Drulović J, Sepčić J, Novaković I, Ristič S, et al. Multiple sclerosis patients carry an increased burden of exceedingly rare genetic variants in the inflammasome regulatory genes. Sci Rep 2019 Jun;9(1):9171.
- 6. Ramos-González E, Bitzer-Quintero O, Ortiz G, Hernández-Cruz J, Ramírez-Jirano L. Relationship between inflammation and oxidative stress and its effect on multiple sclerosis. Neurologia 2024 Apr;39(3):292-301.
- 7. Cui Y, Yu H, Bu Z, Wen L, Yan L, Feng J. Focus on the role of the NLRP3 inflammasome in multiple sclerosis: pathogenesis, diagnosis, and therapeutics. Front Mol Neurosci 2022 May;15:894298.
- 8. Kayagaki N, Stowe IB, Lee BL, O’Rourke K, Anderson K, Warming S, et al. Caspase-11 cleaves gasdermin D for non-canonical inflammasome signalling. Nature 2015 Oct;526(7575):666-671.
- 9. Yi Y-S. Role of inflammasomes in inflammatory autoimmune rheumatic diseases. Korean J Physiol Pharmacol 2018 Jan;22(1):1-15.
- 10. Bernardo-Colón A, Vest V, Clark A, Cooper ML, Calkins DJ, Harrison FE, et al. Antioxidants prevent inflammation and preserve the optic projection and visual function in experimental neurotrauma. Cell Death Dis 2018 Oct;9(11):1097.
- 11. Popa-Wagner A, Mitran S, Sivanesan S, Chang E, Buga A-M. ROS and brain diseases: the good, the bad, and the ugly. Oxid Med Cell Longev 2013;2013:963520.
- 12. Mangan MS, Olhava EJ, Roush WR, Seidel HM, Glick GD, Latz E. Targeting the NLRP3 inflammasome in inflammatory diseases. Nat Rev Drug Discov 2018 Aug;17(8):588-606.
- 13. Niki E, Noguchi N. Antioxidant action of vitamin E in vivo as assessed from its reaction products with multiple biological oxidants. Free Radic Res 2021 Apr;55(4):352-363.
- 14. Pierrot-Deseilligny C, Souberbielle J-C. Contribution of vitamin D insufficiency to the pathogenesis of multiple sclerosis. Ther Adv Neurol Disord 2013 Mar;6(2):81-116.
- 15. Polachini CR, Spanevello RM, Zanini D, Baldissarelli J, Pereira LB, Schetinger MR, et al. Evaluation of delta-aminolevulinic dehydratase activity, oxidative stress biomarkers, and vitamin D levels in patients with multiple sclerosis. Neurotox Res 2016 Feb;29(2):230-242.
- 16. Sintzel MB, Rametta M, Reder AT. Vitamin D and multiple sclerosis: a comprehensive review. Neurol Ther 2018 Jun;7(1):59-85.
- 17. Rao Z, Chen X, Wu J, Xiao M, Zhang J, Wang B, et al. Vitamin D receptor inhibits NLRP3 activation by impeding its BRCC3-mediated deubiquitination. Front Immunol 2019 Dec;10:2783.
- 18. Tulk SE, Liao KC, Muruve DA, Li Y, Beck PL, MacDonald JA. Vitamin D3 metabolites enhance the NLRP3-dependent secretion of IL-1β from human THP-1 monocytic cells. J Cell Biochem 2015 May;116(5):711-720.
- 19. Dapueto R, Rodriguez-Duarte J, Galliussi G, Kamaid A, Bresque M, Batthyány C, et al. A novel nitroalkene vitamin E analogue inhibits the NLRP3 inflammasome and protects against inflammation and glucose intolerance triggered by obesity. Redox Biol 2021 Feb;39:101833.
- 20. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol 2011 Feb;69(2):292-302.
- 21. Jahanbani-Ardakani H, Alsahebfosoul F, Etemadifar M, Abtahi S-H. Interleukin 18 polymorphisms and its serum level in patients with multiple sclerosis. Ann Indian Acad Neurol 2019;22(4):474-476.
- 22. Barclay W, Shinohara ML. Inflammasome activation in multiple sclerosis and experimental autoimmune encephalomyelitis (EAE). Brain Pathol 2017 Mar;27(2):213-219.
- 23. Soares JL, Oliveira EM, Pontillo A. Variants in NLRP3 and NLRC4 inflammasome associate with susceptibility and severity of multiple sclerosis. Mult Scler Relat Disord 2019 Apr;29:26-34.
- 24. Lang Y, Chu F, Shen D, Zhang W, Zheng C, Zhu J, et al. Role of inflammasomes in neuroimmune and neurodegenerative diseases: a systematic review. Mediators Inflamm 2018 Apr;2018:1549549.
- 25. Gandhi F, Jhaveri S, Avanthika C, Singh A, Jain N, Gulraiz A, et al. Impact of vitamin D supplementation on multiple sclerosis. Cureus 2021 Oct;13(10):e18487.
- 26. El-Khateeb M, Khader Y, Batieha A, Jaddou H, Hyassat D, Khawaja N, et al. Vitamin D deficiency and associated factors in Jordan. SAGE Open Med 2019 Sep;7:2050312119876151.
- 27. Chauhan K, Shahrokhi M, Huecker MR. Vitamin D. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC; 2023.
- 28. Salemi G, Gueli MC, Vitale F, Battaglieri F, Guglielmini E, Ragonese P, et al. Blood lipids, homocysteine, stress factors, and vitamins in clinically stable multiple sclerosis patients. Lipids Health Dis 2010 Feb;9(1):19.
- 29. Adamczyk-Sowa M, Galiniak S, Żyracka E, Grzesik M, Naparło K, Sowa P, et al. Oxidative modification of blood serum proteins in multiple sclerosis after interferon beta and melatonin treatment. Oxid Med Cell Longev 2017:7905148.
- 30. Muhammed O, Al-Rubae’i S. Role of antioxidant and oxidative stress levels in multiple sclerosis Iraqi patients. Journal of Physics: Conference Series; 2021: IOP Publishing.
- 31. Yakout SM, Alfadul H, Ansari MG, Khattak MN, Al-Daghri NM, Vitamin D. Vitamin D status modestly regulates NOD-like receptor family with a pyrin domain 3 inflammasome and interleukin profiles among Arab adults. Int J Mol Sci 2023 Nov;24(22):16377.
- 32. van Tits LJ, Demacker PN, de Graaf J, Hak-Lemmers HL, Stalenhoef AF. α-tocopherol supplementation decreases production of superoxide and cytokines by leukocytes ex vivo in both normolipidemic and hypertriglyceridemic individuals. Am J Clin Nutr 2000 Feb;71(2):458-464.
- 33. Roffe-Vazquez DN, Huerta-Delgado AS, Castillo EC, Villarreal-Calderón JR, Gonzalez-Gil AM, Enriquez C, et al. Correlation of vitamin d with inflammatory cytokines, atherosclerotic parameters, and lifestyle factors in the setting of heart failure: a 12-month follow-up study. Int J Mol Sci 2019 Nov;20(22):5811.
- 34. Noroozi S, Meimand HA, Arababadi MK, Nakhaee N, Asadikaram G. The effects of IFN-β 1a on the expression of inflammasomes and apoptosis-associated speck-like proteins in multiple sclerosis patients. Mol Neurobiol 2017 May;54(4):3031-3037.