The Global Cancer Observatory estimated that 1.9 million new colorectal cancer (CRC) incident cases and 935 000 deaths occurred in 2020, representing 10% of all cancer diagnoses and mortality, making CRC the second leading cause of cancer death worldwide.1 The Global Burden of Disease (GBD) study estimated that the CRC incident and death cases increased by more than 50% in most world regions from 1990 to 2019.2 Despite the increase in the total number of CRC deaths, the global age-standardized mortality rate (ASMR) decreased from 14.3 per 100 000 in 1990 to 13.7 per 100 000 in 2019.
In contrast to the global trend, the CRC ASMR in the North Africa and Middle East (NAME) region is increasing.2,3 The GBD study estimated that the total number of deaths due to CRC increased by 199% in the region, while ASMRs increased by 20% during the last three decades.
The GBD study, along with research from numerous NAME countries, has highlighted the increasing burden of colorectal cancer (CRC) across the region.4—15 In Oman, CRC was the third most common cancer in women, and the fourth most common cancer in men in 2015.12 By 2019, with a clear upward trend, CRC had become the most common cancer among Omani men, and remained the third most common cancer among Omani women in 2019.5,13 In Saudi Arabia, CRC mortality increased by four-fold in men and three-fold in women between 1990 and 2019.6 A study of the Lebanese National Cancer Registry showed that CRC age-standardized incidence rate increased from 16.3 to 23.2 per 100 000 in men, and from 13.0 to 20.2 per 100 000 in women between 2005 and 2016.7 In Iraq, CRC incidence rose by approximately 81% between 2008 and 2016.14 An analysis of the Iraqi National Cancer Registry estimated annual percent changes of 5.1% for CRC incidence and 3.5% for CRC mortality between 2000 and 2019.8 In Jordan, CRC was the second most common cancer during the 2000–2013 period, with noticeable increasing age-standardized incidence rate.11 In Tunisia, CRC incidence increased from 6.4 per 100 000 to 12.4 per 100 000 between 1994 and 2009.9 Similarly, in Turkey, CRC is among the most common cancers, showing an increasing incidence trend.10,15
A recent analysis of the GBD study suggested that the CRC burden in the NAME region is increasing at a faster pace compared to other regions in the world.3 The increase could be linked to changes in behavioral, dietary, and metabolic risk factors.3,16
While the upward trend of the CRC mortality in the NAME region is evident, the key drivers of this increase are still not fully established. To examine the impact of risk factors on the rise of CRC mortality, we calculated changes in risk-related ASMR in the NAME region between 1990 and 2019 for 11 GBD risk factors.
Methods
The GBD study, led by the Institute for Health Metrics and Evaluation, is a global epidemiological database that provides incidence, prevalence, mortality, and disability estimates across 369 diseases in 204 countries. These countries are grouped into 21 regions and seven super-regions, including: Central Europe, Eastern Europe, and Central Asia; high-income region; Latin America and Caribbean; South Asia; Southeast Asia, East Asia, and Oceania; Sub-Saharan Africa; and NAME, which is the focus of this study.2,17,18 The NAME region consists of 21 countries [Table 1].
Table 1: Colorectal cancer age-standardized mortality rates in the North Africa and Middle East, 1990–2019.
|
North Africa and Middle East region
|
8.2, 9.8 (19.5)
|
8.4, 10.5 (25.0)
|
7.9, 9.2 (16.5)
|
|
Afghanistan
|
7.9, 8.4 (6.3)
|
7.5, 8.0 (6.7)
|
8.2, 8.9 (8.5)
|
|
Algeria
|
7.2, 8.0 (11.1)
|
7.3, 8.1 (11.0)
|
7.2, 8.1 (12.5)
|
|
Bahrain
|
12.4, 11.4 (-8.1)
|
14.8, 12.9 (-12.8)
|
10.4, 9.9 (-4.8)
|
|
Egypt
|
5.5, 7.4 (34.5)
|
5.2, 7.3 (40.4)
|
5.6, 8.0 (42.9)
|
|
Iran
|
7.2, 9.3 (29.2)
|
7.6, 10.2 (34.2)
|
6.6, 8.4 (27.3)
|
|
Iraq
|
7.2, 8.3 (15.3)
|
7.9, 9.5 (20.3)
|
6.6, 7.3 (10.6)
|
|
Jordan
|
12.4, 13.1 (5.6)
|
12.4, 14.1 (13.7)
|
12.5, 12.0 (-4.0)
|
|
Kuwait
|
7.4, 10.1 (36.5)
|
6.4, 11.7 (82.8)
|
8.7, 7.9 (-9.2)
|
|
Lebanon
|
13.4, 17.6 (31.3)
|
13.6, 19.6 (44.1)
|
13.3, 15.9 (19.5)
|
|
Libya
|
11.9, 12.5 (5.0)
|
11.3, 12.2 (8.0)
|
12.8, 12.7 (-0.8)
|
|
Morocco
|
6.3, 8.5 (34.9)
|
6.1, 8.8 (44.3)
|
6.4, 8.2 (28.1)
|
|
Oman
|
7.7, 10.2 (32.5)
|
7.3, 10.1 (38.4)
|
8.3, 10.6 (27.7)
|
|
Palestine
|
14.8, 19.6 (32.4)
|
16.4, 23.1 (40.9)
|
13.5, 17.3 (28.1)
|
|
Qatar
|
14, 16.5 (17.9)
|
10.5, 13.7 (30.5)
|
18.6, 25.9 (39.2)
|
|
Saudi Arabia
|
6.8, 9.7 (42.6)
|
6.4, 9.5 (48.4)
|
7.3, 9.9 (35.6)
|
|
Sudan
|
5.0, 7.1 (42.0)
|
5.1, 7.5 (47.1)
|
5.0, 6.6 (32.0)
|
|
Syria
|
5.5, 6.3 (14.5)
|
5.4, 6.4 (18.5)
|
5.7, 6.4 (12.3)
|
|
Tunisia
|
8.1, 9.7 (19.8)
|
7.6, 10.0 (31.6)
|
8.6, 9.5 (10.5)
|
|
Turkey
|
13.2, 13.1 (-0.8)
|
14.7, 15.6 (6.1)
|
11.9, 10.9 (-8.4)
|
|
UAE
|
18.5, 17.4 (-5.9)
|
19.8, 18.4 (-7.1)
|
18, 14.9 (-17.2)
|
The GBD database compiles data from censuses, national surveys, registries, vital statistics, published research articles, and other sources. When primary data is unavailable, modeling is used to estimate values. For CRC, data are obtained from vital registration (birth, death, cause of death) and cancer registries.4 When the vital registration is unavailable or incomplete, cause-of-death information is collected through verbal autopsies, where trained interviewers obtained clinical and demographic information about the recently deceased from relatives.
CRC data sources for the NAME region are accessible via the GBD Data Input Sources Tool (https://ghdx.healthdata.org/gbd-2019/data-input-sources). We conducted a search on 23 January 2025, using the following criteria: Components = “cause of death”, causes = “colon and rectum cancer”, location = “North Africa and Middle East”. The search identified 220 source reports related to NAME CRC data, mainly from ministries of health, national vital registrations, and cancer registries. Detailed descriptions of the data collection are provided in previous GBD study publications.2,4,17,18
Data on CRC mortality and risk factors in the NAME region and countries were retrieved using the GBD study online query tool (https://vizhub.healthdata.org/gbd-results/). We extracted estimates of the overall ASMR, as well as ASMR attributed to 11 risk factors, stratified by sex and country.
In this study, we analyzed ASMR data obtained from the GBD database. All rates were reported per 100 000 person-years.19 We also included in the analysis risk-related ASMRs. To estimate the risk-related burden of diseases, the GBD identifies risk factors based on World Cancer Research Fund criteria and plausible evidence.2 The relative risk of each factor is estimated by the GBD study through meta-analyses as a function of exposure.2,18 Exposure to risk factors is determined by the GBD study through a systematic search of published studies, surveys, censuses, administrative reports, and other sources. The exposure to risk factor is estimated for age-sex-location-year groups using various methods, primarily Bayesian models. The population attributable fraction is then calculated by age-sex-location-year group and applied to estimate the CRC burden and ASMR attributed to each risk factor. More details on the incidence and mortality rates estimation are provided in the GBD study publications.2,4,17,19,20
Eleven risk factors contributing to CRC mortality are included in the GBD study. These factors are divided into two main categories: behavioral risks including alcohol use, low physical activity, tobacco (smoking), and dietary risks (diet low in whole grains, diet low in milk, diet high in red meat, diet high in processed meat, diet low in fiber, diet low in calcium), and metabolic risks including high fasting plasma glucose (FPG) and high body mass index (BMI).1,2 ASMR per 100 000 and ASMR proportions related to each risk factor were analyzed to examine the impact of risk factors on the CRC burden.
Descriptive analysis was performed on the CRC mortality rate (ASMR) data. Rate changes (ΔASMR) were calculated by computing the differences between the 2019 and 1990 rates. Percent changes were calculated by subtracting 100% from the rate ratios. Analyses were executed using the R statistical software version 4.3.2.
Results
In the NAME region, CRC ASMR increased by 19.5% (ASMRΔ = 1.6) between 1990 and 2019 [Table 1]. ASMR increased in all NAME countries except Bahrain, the UAE, and Turkey, with the highest increase observed in Saudi Arabia (42.6%). CRC ASMR increased by 25.0% (ΔASMR = 2.1) in men. Increases were observed in all countries except Bahrain and the UAE, with the highest increase in Kuwait (82.8%).
In the female population, CRC ASMR increased by 16.5% (ΔASMR = 1.3). Increases were seen in 15 countries, with the largest in Egypt (42.9%).
Analysis of risk-attributed ASMR changes between 1990 and 2019 showed that high FPG and high BMI had the largest ΔASMR values (0.56 and 0.55, respectively) across the population [Table 2]. In men, the highest ΔASMR was linked to high BMI (0.85), followed by high FPG (0.62) and diet low in whole grains (0.39). In women, the highest ΔASMR was linked to high FPG (0.50), followed by diet low in whole grains (0.25) and high BMI (0.24).
Table 2: Colorectal cancer age-standardized mortality rates (ASMR) related to risk factors in the North African and Middle East population, 1990–2019.
|
Alcohol use
|
0.09
|
0.10
|
0.01
|
11.1
|
0.14
|
0.16
|
0.02
|
14.3
|
0.04
|
0.04
|
0.00
|
0.0
|
|
Low physical activity
|
0.77
|
1.03
|
0.26
|
33.9
|
0.81
|
1.12
|
0.31
|
38.3
|
0.72
|
0.95
|
0.23
|
31.9
|
|
Smoking
|
1.00
|
1.14
|
0.14
|
14.0
|
1.76
|
1.98
|
0.22
|
12.5
|
0.26
|
0.28
|
0.02
|
7.7
|
|
Diet high in processed meat
|
0.07
|
0.10
|
0.03
|
42.9
|
0.07
|
0.1
|
0.03
|
42.9
|
0.07
|
0.10
|
0.03
|
42.9
|
|
Diet high in red meat
|
0.18
|
0.22
|
0.04
|
22.2
|
0.19
|
0.23
|
0.04
|
21.1
|
0.18
|
0.20
|
0.02
|
11.1
|
|
Diet low in calcium
|
1.28
|
1.32
|
0.04
|
3.1
|
1.39
|
1.51
|
0.12
|
8.6
|
1.17
|
1.14
|
-0.03
|
-2.6
|
|
Diet low in fiber
|
0.07
|
0.08
|
0.01
|
14.3
|
0.07
|
0.08
|
0.01
|
14.3
|
0.07
|
0.07
|
0.00
|
0.0
|
|
Diet low in milk
|
1.27
|
1.55
|
0.28
|
22.0
|
1.3
|
1.65
|
0.35
|
26.9
|
1.23
|
1.45
|
0.22
|
17.9
|
|
Diet low in whole grains
|
1.66
|
1.98
|
0.32
|
19.3
|
1.71
|
2.1
|
0.39
|
22.8
|
1.60
|
1.85
|
0.25
|
15.6
|
|
High body mass index
|
0.62
|
1.17
|
0.55
|
88.7
|
0.83
|
1.68
|
0.85
|
102.4
|
0.41
|
0.65
|
0.24
|
58.5
|
Figure 1 illustrates the trends of risk-related CRC ASMR in men and women between 1990 and 2019.
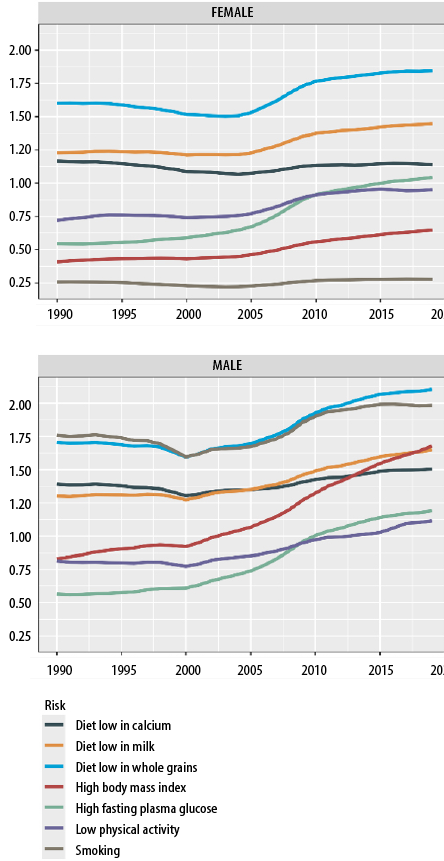 Figure 1: Trends of colorectal cancer age-standardized mortality rates per 100 000 for the top seven risk factors from 1990 to 2019.
Figure 1: Trends of colorectal cancer age-standardized mortality rates per 100 000 for the top seven risk factors from 1990 to 2019.
To examine the total effect of all metabolic risk factors (high FPG and high BMI) on the CRC mortality increase, we calculated the change in ASMR attributed to metabolic risks. In the general NAME population, ASMR attributed to metabolic risks increased by 1.03 (from 1.13 to 2.16), a 91.2% rise. In men, the risk increased by 1.34 (from 1.34 to 2.68), a 100% rise. In women, the metabolic risk-related ASMR increased by 0.70 (from 0.92 to 1.62), a 76.1% rise. To examine the relative effect of metabolic risk factors on the CRC mortality increase, we calculated the proportion of metabolic risk-related ΔASMR of the total ASMR change. Metabolic risk-related ΔASMR accounted for 64.4% (1.03/1.60) of the total CRC mortality increase in the region, 63.8% (1.34/2.10) of the increase in men, 53.8% (0.70 / 1.30) of the increase in women.
Discussion
This study analyzed CRC mortality in the NAME region between 1990 and 2019 using GBD study data. Our results show a marked rise in CRC ASMR, largely explained by metabolic risk factors, particularly high BMI and high FPG. In general, males were more affected than females with the CRC burden. The upward trend in mortality was also more evident in the male population. Recent epidemiological studies have shown that the CRC burden and mortality are increasing in the NAME region.2–4,16 Our results suggest that metabolic factors (hyperglycemia and obesity) are the main contributors to the rise in CRC mortality in the region. The total effect of metabolic risks explained a significant proportion (about 64.4%) of the CRC mortality increase.
Clinically, obesity is associated with higher mortality rates due to CRC and cancer in general, as well as poor prognosis in CRC patients.21,22 Globally, high BMI alone accounts for approximately 3.9% of all cancer cases.23 In a meta-analysis of observational studies, Doleman et al.,22 found that obese individuals have 14% increased risk of CRC mortality, and 7% increased risk of recurrence compared to individuals with normal weight. Additionally, it is estimated that diabetes alone accounts for 2.1% of all cancer cases worldwide.23 In a large cohort study in the USA, type 2 diabetes was associated with a 47% increased risk of CRC.24 Moreover, studies suggest that patients with type 2 diabetes have at least 20% higher risk of cancer-related death.25
Adiposity and hyperglycemia can increase the risk of CRC through multiple mechanisms , such as low-grade inflammation, oxidative stress, hyperinsulinemia, alterations in the concentration of the insulin-like growth factor (IGF) and cytokines, such as interleukin (IL)-6, IL-1β, and tumor necrosis factor-α, promoting cancer cells' growth and survival.26–30 Additionally, hyperglycemia provides excess energy to cancer cells, aiding their growth.31 It can also increase the production of free radicals leading to DNA damage and enhancing metastasis. Higher insulin levels, seen in type 2 diabetes, also increase the risk of cancer.32 Binding of insulin to the insulin receptors activates the phosphoinositide 3-kinase/Akt/mTOR signaling pathway, promoting cellular proliferation and survival. Bouras et al,29 suggested that plasma IGF1 could partially explain the mechanism by which high BMI increases the risk of CRC. IGF1 binds to the IGF1R receptors, activating intracellular kinase signaling pathways including the mitogen-activated protein kinase and phosphoinositide 3-kinase, and stimulating cellular growth.30,32 IGF1R receptors are extensively present in the proliferating cells of the colonic crypts. Furthermore, IGF1R receptors have been found to be overexpressed in human CRC tissues. IGF1 also contributes to the Warburg effect, a phenomenon in which cancer cells switch to aerobic glycolysis for energy production and growth.
Dysregulation of the immune system may also affect the development and prognosis of cancer in obese patients. In mice, obesity has been shown to affect the level of IL-10, an important immune modulator.33 Some studies suggested that the IL-10 levels are associated with cancer stage.34,35 The role of IL-10 in cancer development and progression remains unclear, with possible protective and harmful effects, and needs further evaluation. Transforming growth factor (TGF)-β is another cytokine that regulates immunity, fibrosis, and cell proliferation.36 The role of TGF-β has been studied in breast, colorectal, pancreatic, lung, and hematologic malignancies.36,37 Two opposing roles for TGF-β in cancer formation were identified: one inhibiting tumor growth and the other promoting tumor progression.36 In its role promoting cancer, TGF- β plays a significant role in inflammation suppression. However, excessive activation of TGF-β can lead to immune suppression, creating an environment that favors cancer development. In CRC, high TGF-β activation has been observed in tumor stroma contributing to tumor metastasis.38,39 TGF-β can be increased in obese patients due to chronic elevation of the tumor necrosis factor-α.40 Toll-like receptors (TLR) and programmed death-ligand 1 (PD-L1) are other immune components that are involved in cancer development. TLR4 and TLR2 have a crucial role in the defense against infections and recognition of microorganisms.33,41 However, overexpression of TLR4 is associated with poor prognosis in CRC patients.42 Hu et al,43 reported that TLR4 promoted CRC growth in mice fed with a high-fat diet. PD-L1 expression is also associated with poor prognosis in cancer patients.44,45 Obesity can enhance the PD-L1 expression via the IL6/JAK/STAT pathway.46
Our findings have important implications regarding the prevention and control of CRC in the NAME region. Interventions targeting CRC prevention and control should essentially consider targeting obesity and hyperglycemia. Regional and national interventions could include educational campaigns, providing nutritional information to consumers, economic incentives, legislative measures, and other strategic approaches.4 It is crucial to establish and enhance cancer registries, health surveys, and research programs that assess nutritional, metabolic, and health conditions in NAME countries. Such surveys and data from the NAME countries remain widely unavailable.47 Additionally, clinical studies to investigate the effect of metabolic risk factors on the CRC patients’ prognosis, quality of life, and response to treatment are needed in the region. The interaction between metabolic risks and biological factors, like genetic variation and biomarkers, is another area to be explored.
The limitations of GBD studies have been reported previously.2,4,17 The main limitations of GBD are the inaccuracy and unavailability of data from some countries, underreporting of cancer cases, and detection bias. In this study, we wanted to compare homogenized quantities between populations that have different age distributions. We used the age-standardized rates to eliminate the effect of different age structures across populations and time points. The main limitation of age-standardization is obscuring the actual rates and true disease burden.48 One way to avoid this limitation is to use age-specific rates. However, using age-specific rates was beyond the scope of this study. Future studies are needed to address this concern. Another concern is that the GBD definition of risk factor may include a range of exposure levels, each with different levels of association with CRC mortality. For example, high FPG was defined by the GBD as any glucose level higher than the theoretical minimum risk exposure level of 4.8–5.4 mmol/L.49 Using this definition, the high FPG risk exposure can encompass both diabetic (FPG ≥ 7.0 mmol/L), regardless of whether they are on antidiabetic management, and non-diabetic individuals. In the current study, we could not assess the impact of higher FPG levels, such as those seen in uncontrolled diabetic patients, on the CRC burden. Additionally, without clinical data, we were unable to determine the potential beneficial effect of antidiabetic treatments on the reduction of the CRC burden.
Despite these limitations, this study provides key findings regarding the role of metabolic factors in increasing the CRC burden in the NAME region and highlights the importance of monitoring the metabolic conditions and their impact on public health. Our findings demonstrate that metabolic factors (high BMI and high FPG) are the major contributors to the rising CRC mortality. Reducing the exposure to these risk factors is crucial. Public education on the impacts of high BMI and high FPG is essential. Targeted public health campaigns to modify behavioral and dietary habits, related to these factors, are urgently needed in the region.
Conclusion
Our study showed that the rising burden of CRC in the NAME region is mainly driven by metabolic factors, particularly high FPG and high BMI. Targeted interventions addressing these risk factors in the NAME countries are urgently needed.
Disclosure
The authors declare no conflicts of interest. No funding was received for this study.
references
- 1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021 May;71(3):209-249.
- 2. GBD 2019 Colorectal Cancer Collaborators. Global, regional, and national burden of colorectal cancer and its risk factors, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Gastroenterol Hepatol 2022 Jul;7(7):627-647.
- 3. Haghighatdoost F, Mehrabani-Zeinabad K, Hajihashemi P, Mohammadifard N, Adibi P. Burden of colorectal cancer and its risk factors in the North Africa and Middle East (NAME) region, 1990-2019: a systematic analysis of the global burden of disease study. BMC Public Health 2024 Feb;24(1):557.
- 4. GBD 2017 Colorectal Cancer Collaborators. The global, regional, and national burden of colorectal cancer and its attributable risk factors in 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol 2019 Dec;4(12):913-933.
- 5. Al-Sayegh H, Al-Zadjali S, Al-Moundhri M. Analyzing cancer incidence trends in Oman from 1996 to 2019: a comprehensive study of the national cancer annual reports. JCO Glob Oncol 2024 Jan;10:e2300337.
- 6. Ghulam E, Ramadan M. Age-period-cohort analysis of colorectal cancer mortality in Saudi Arabia from 1990 to 2019. Public Health 2024 Mar;228:43-50.
- 7. Lakkis NA, El-Kibbi O, Osman MH. Colorectal cancer in Lebanon: incidence, temporal trends, and comparison to regional and western countries. Cancer Control 2021;28:1073274821996869.
- 8. Ibrahem S, Ahmed H, Zangana S. Trends in colorectal cancer in Iraq over two decades: incidence, mortality, topography and morphology. Ann Saudi Med 2022;42(4):252-261.
- 9. Khiari H, Ben Ayoub HW, Ben Khadhra H, Hsairi M. Colorectal cancer incidence trend and projections in Tunisia (1994 - 2024). Asian Pac J Cancer Prev 2017 Oct;18(10):2733-2739.
- 10. Seydaoğlu G, Özer B, Arpacı N, Parsak CK, Eray IC. Trends in colorectal cancer by subsite, age, and gender over a 15-year period in Adana, Turkey: 1993-2008. Turk J Gastroenterol 2013;24(6):521-531.
- 11. Khader YS, Sharkas GF, Arkoub KH, Alfaqih MA, Nimri OF, Khader AM. The epidemiology and trend of cancer in Jordan, 2000-2013. J Cancer Epidemiol 2018 Oct;2018:2937067.
- 12. Al-Lawati NA, Al-Bahrani BJ, Al-Raisi SS, Al-Lawati JA. Twenty-year trends of cancer incidence in Omanis, 1996-2015. Oman Med J 2019 Jul;34(4):361-387.
- 13. Ministry of Health. Cancer incidence in Oman. 2019 [cited 2025 Jan 27]. Available from: https://www.moh.gov.om/en/statistics/cancer-repoerts/cancer-incidence-in-oman-2019/.
- 14. Hussain AM, Lafta RK. Cancer trends in Iraq 2000-2016. Oman Med J 2021 Jan;36(1):e219.
- 15. Celikgun S, Nur N. Cancer incidence rates by age and gender in Sivas province of Turkey, 2004-2014. Oman Med J 2019 Mar;34(2):126-130.
- 16. Pasdar Y, Shadmani FK, Fateh HL, Soleimani D, Hamzeh B, Ghalandari M, et al. The burden of colorectal cancer attributable to dietary risk in Middle East and North African from 1990 to 2019. Sci Rep 2023 Nov;13(1):20244.
- 17. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Lond Engl 2020 Oct;396(10258):1204-1222.
- 18. Murray CJ, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Lond Engl 2020 Oct;396(10258):1223-1249.
- 19. Global Burden of Disease Collaborative Network. Global burden of disease study 2019 (GBD 2019) data resources | GHDx. [cited 2024 Mar 6]. Available from: https://ghdx.healthdata.org/gbd-2019.
- 20. Global Burden of Disease Collaborative Network. Global burden of disease study 2019 (GBD 2019) socio-demographic index (SDI) 1950–2019. Institute for Health Metrics and Evaluation (IHME); 2020 [cited 2024 Jan 30]. Available from: https://ghdx.healthdata.org/record/ihme-data/gbd-2019-socio-demographic-index-sdi-1950-2019.
- 21. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 2003 Apr;348(17):1625-1638.
- 22. Doleman B, Mills KT, Lim S, Zelhart MD, Gagliardi G. Body mass index and colorectal cancer prognosis: a systematic review and meta-analysis. Tech Coloproctol 2016 Aug;20(8):517-535.
- 23. Pearson-Stuttard J, Zhou B, Kontis V, Bentham J, Gunter MJ, Ezzati M. Worldwide burden of cancer attributable to diabetes and high body-mass index: a comparative risk assessment. Lancet Diabetes Endocrinol 2018 Jun;6(6):e6-e15.
- 24. Lawler T, Walts ZL, Steinwandel M, Lipworth L, Murff HJ, Zheng W, et al. Type 2 diabetes and colorectal cancer risk. JAMA Netw Open 2023 Nov;6(11):e2343333.
- 25. de Andrade Mesquita L, Wayerbacher LF, Schwartsmann G, Gerchman F. Obesity, diabetes, and cancer: epidemiology, pathophysiology, and potential interventions. Arch Endocrinol Metab 2023 Jun;67(6):e000647.
- 26. Aleksandrova K, Nimptsch K, Pischon T. Influence of obesity and related metabolic alterations on colorectal cancer risk. Curr Nutr Rep 2013 Mar;2(1):1-9.
- 27. Xu J, Ye Y, Wu H, Duerksen-Hughes P, Zhang H, Li P, et al. Association between markers of glucose metabolism and risk of colorectal cancer. BMJ Open 2016 Jun;6(6):e011430.
- 28. Kasprzak A. Insulin-like growth factor 1 (IGF-1) signaling in glucose metabolism in colorectal cancer. Int J Mol Sci 2021 Jun;22(12):6434.
- 29. Bouras E, Gill D, Zuber V, Murphy N, Dimou N, Aleksandrova K, et al. Identification of potential mediators of the relationship between body mass index and colorectal cancer: a Mendelian randomization analysis. Int J Epidemiol 2024 Apr;53(3):dyae067.
- 30. Gligorijević N, Dobrijević Z, Šunderić M, Robajac D, Četić D, Penezić A, et al. The insulin-like growth factor system and colorectal cancer. Life (Basel) 2022 Aug;12(8):1274.
- 31. Wang M, Yang Y, Liao Z. Diabetes and cancer: epidemiological and biological links. World J Diabetes 2020 Jun;11(6):227-238.
- 32. Kim DS, Scherer PE. Obesity, diabetes, and increased cancer progression. Diabetes Metab J 2021 Nov;45(6):799-812.
- 33. Yang PK, Chou CH, Huang CC, Wen WF, Chen HF, Shun CT, et al. Obesity alters ovarian folliculogenesis through disrupted angiogenesis from increased IL-10 production. Mol Metab 2021 Jul;49:101189.
- 34. Mohammed DA, Khallaf SM, El-Naggar MG, Abdel-Hameed MR, Bakry R. Interleukin-10: a potential prognostic marker in patients with newly diagnosed multiple myeloma. Resum Oncol 2021 Jun;17(1):38-41.
- 35. Dwivedi S, Goel A, Natu SM, Mandhani A, Khattri S, Pant KK. Diagnostic and prognostic significance of prostate specific antigen and serum interleukin 18 and 10 in patients with locally advanced prostate cancer: a prospective study. Asian Pac J Cancer Prev 2011;12(7):1843-1848.
- 36. Massagué J, Sheppard D. TGF-β signaling in health and disease. Cell 2023 Sep;186(19):4007-4037.
- 37. Abdel Hammed MR, Ahmed YA, Adam EN, Bakry R, Elnaggar MG. sVCAM-1, and TGFβ1 in chronic phase, chronic myeloid leukemia patients treated with tyrosine kinase inhibitors. Egypt J Immunol 2022 Oct;29(4):163-173.
- 38. Peng D, Fu M, Wang M, Wei Y, Wei X. Targeting TGF-β signal transduction for fibrosis and cancer therapy. Mol Cancer 2022 Apr;21(1):104.
- 39. Calon A, Espinet E, Palomo-Ponce S, Tauriello DV, Iglesias M, Céspedes MV, et al. Dependency of colorectal cancer on a TGF-β-driven program in stromal cells for metastasis initiation. Cancer Cell 2012 Nov;22(5):571-584.
- 40. Samad F, Uysal KT, Wiesbrock SM, Pandey M, Hotamisligil GS, Loskutoff DJ. Tumor necrosis factor alpha is a key component in the obesity-linked elevation of plasminogen activator inhibitor 1. Proc Natl Acad Sci U S A 1999 Jun;96(12):6902-6907.
- 41. Abdel Hammed MR, Elgendy SG, El-Mokhtar MA, Sayed D, Mansour SM, Darwish AM. T-lymphocytes expression of toll-like receptors 2 and 4 in acute myeloid leukemia patients with invasive fungal infections. Mediterr J Hematol Infect Dis 2022 Mar;14(1):e2022022.
- 42. Cammarota R, Bertolini V, Pennesi G, Bucci EO, Gottardi O, Garlanda C, et al. The tumor microenvironment of colorectal cancer: stromal TLR-4 expression as a potential prognostic marker. J Transl Med 2010 Nov;8:112.
- 43. Hu X, Fatima S, Chen M, Xu K, Huang C, Gong RH, et al. Toll-like receptor 4 is a master regulator for colorectal cancer growth under high-fat diet by programming cancer metabolism. Cell Death Dis 2021 Aug;12(8):791.
- 44. Abdel Hafeez L, Mansor S, Zahran A, Hamed H, Abdel Hameed M, Bakry R. Expression of programmed death ligand-1 (PDL-1) in acute myeloid leukemia patients and its relation to post induction response. SECI Oncol J 2021 Apr;9(2):106-111.
- 45. Wu P, Wu D, Li L, Chai Y, Huang J. PD-L1 and survival in solid tumors: a meta-analysis. PLoS One 2015 Jun;10(6):e0131403.
- 46. Wang Y, Zhang X, Xie X, Chen W, Li M, Diao D, et al. Obesity and metabolic syndrome related macrophage promotes PD-L1 expression in TNBC through IL6/JAK/STAT pathway and can be reversed by telmisartan. Cancer Biol Ther 2020 Dec;21(12):1179-1190.
- 47. Hammerich A, Fouad H, Rashidian A, Hajjeh R, Al Mandhari A. Enhancing the quality and accuracy of national cancer registries in the Eastern Mediterranean Region. East Mediterr Health J 2023 Aug;29(8):603-604.
- 48. Thurber KA, Thandrayen J, Maddox R, Barrett EM, Walker J, Priest N, et al. Reflection on modern methods: statistical, policy and ethical implications of using age-standardized health indicators to quantify inequities. Int J Epidemiol 2022 Feb;51(1):324-333.
- 49. Moradi-Lakeh M, Forouzanfar MH, El Bcheraoui C, Daoud F, Afshin A, Hanson SW, et al; Global Burden of Disease Collaborators on Eastern Mediterranean Region and Diabetes. High fasting plasma glucose, diabetes, and its risk factors in the Eastern Mediterranean Region, 1990-2013: findings from the global burden of disease study 2013. Diabetes Care 2017 Jan;40(1):22-29.