Child maltreatment is a global public health concern with long-term consequences on individuals, families, and communities. It encompasses various forms of violence, including physical, sexual, and emotional abuse, as well as neglect.1
The Adverse Childhood Experience study has extensively documented the immediate and long-term impacts of child maltreatment on mental and physical health.2
The United Nations has designated Sustainable Development Goals Target 16.2 as the goal to end all forms of violence against children, and includes key indicators to monitor its progress.3 In May 2021, the World Health Assembly passed a resolution urging member states to strengthen health systems to prevent, identify, and respond to violence against children.4 Healthcare professionals play a vital role in child protection, particularly in terms of identifying, detecting, and providing health services to children and their families.5
Since the Sustainable Development Goals’ adoption in 2015, countries have taken action to prevent and respond to violence against children. In Oman, cases of child maltreatment were recognized by healthcare professionals as early as the 1990s.6,7 The Ministry of Health (MOH) formally introduced national child protection policies in 2006. This paper provides an overview of Oman’s progress in child protection, focusing on the role of healthcare and benchmarking efforts against the World Health Organization’s (WHO) 2016 INSPIRE strategy, which outlines a comprehensive approach to child protection: Implementation and law enforcement, Norms and values, Safe environments, Parent and caregiver support, Income and economy, Response and support services, and Education and life skills (INSPIRE).
Methods
We conducted a literature review of the period from 2000 to 2024 on child maltreatment in Oman. Sources included Google Scholar, PubMed, and other search engines, along with official government reports, policies, and unpublished expert reports. Keywords such as “child abuse,” “child negligence,” “child maltreatment,” and “child protection” were used. The role of the MOH.
Healthcare professionals play a crucial role in identifying and responding to child maltreatment.8 In Oman, their contributions have been instrumental in recognizing child maltreatment as a public health concern and shaping relevant strategies.
The Sixth Cycle of Planning in 2006 incorporated child maltreatment into the Child Health Domain, aiming to measure reported cases at health facilities.
A dedicated task force, comprising members from MOH, the Royal Hospital, and Sultan Qaboos University, developed and piloted a child maltreatment reporting system, which was officially launched in 2010.9 This task force has been pivotal in raising awareness, training healthcare providers, and creating a national database to assess the extent of child maltreatment in Oman. Data collected are used to guide national policies and increase commitment among policymakers. Figure 1 outlines the processes and procedures for reporting child maltreatment incidents that come to the attention of healthcare facilities.
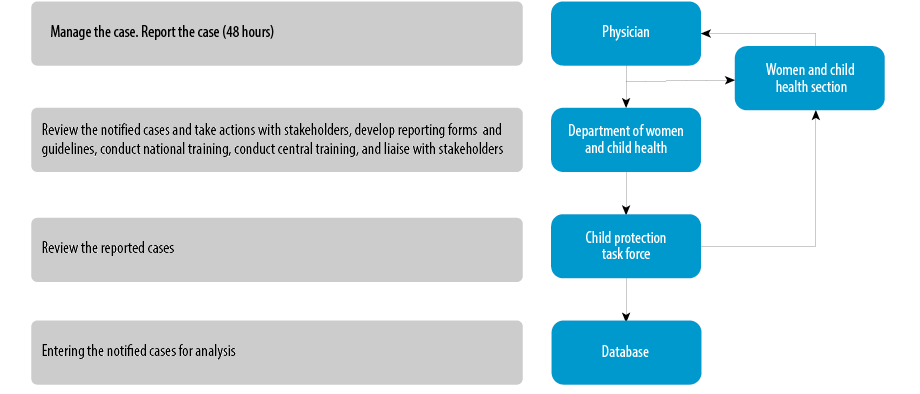 Figure 1: Reporting algorithm system of child maltreatment cases reaching healthcare facilities.
Figure 1: Reporting algorithm system of child maltreatment cases reaching healthcare facilities.
In addition, multi-sectoral Child Protection Committees (CPCs) were established, involving stakeholders from the MOH, Ministry of Social Development (MOSD), Ministry of Education, Ministry of Justice and Legal Affairs, Ministry of Labor, Royal Oman Police, and non-governmental organizations. The MOSD launched a national child protection hotline in 2010 for reporting cases. 9
While numerous laws in Oman address child protection concerns, it was important to have a law specifically for children. The Omani Child’s Law, which is comprehensive and addresses all child rights, was ratified in May 2014. Specific provisions of the law (175, Omani Child Law)1 mandate the mandatory reporting of child maltreatment and the punitive punishment of offenders.
The INSPIRE Strategy
The INSPIRE strategy aims to address child maltreatment using a set of seven measures that have shown efficacy. The strategy is a joint initiative between several agencies, including the WHO, UNICEF, the World Bank, USAID, NDC, and UNODC. Each INSPIRE strategy [Figure 2] includes a list of evidence-based approaches that have shown effectiveness in reducing violence against children either by modifying risk factors or mitigating consequences.5 The sections below outline each strategy and detail the relevant efforts made in Oman.
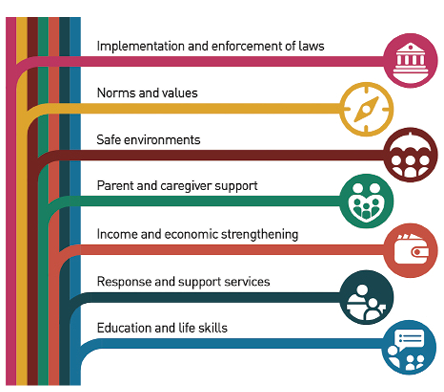 Figure 2: INSPIRE Strategy for ending violence against children.
Figure 2: INSPIRE Strategy for ending violence against children.
- Implementation and enforcement of law
Oman ratified the Convention on the Rights of the Child in 1986, ensuring free access to education and healthcare. In 2014, Oman enacted a comprehensive Child Law, mandating the reporting of child maltreatment and establishing CPCs. These committees, operational at both regional and central levels throughout all eleven Sultanate regions, are authorized to receive complaints and intervene in cases of violence
or neglect.
- Norms and values
Oman has aligned its definition of child maltreatment with WHO standards, with minor adjustments to accommodate the specific circumstances including certain harmful indigenous customs.10 The WHO defined child maltreatment as “all forms of physical, emotional, sexual abuse, neglect, negligent treatment, and exploitation resulting in actual or potential harm to the child’s health, survival, development, or dignity in the context of a relationship of responsibility, trust, or power”.10 Harmful practices such as female genital mutilation and child marriage (before age 18) have been prohibited.
The UNICEF Oman Country Office introduced the Social and Behavior Change (SBC) strategy to shift societal attitudes toward non-violent child-rearing practices. This strategy is based on the Social-Ecological Model, which involves understanding the multiple levels of a system and the interactions between individuals and their environment within it to ensure the greatest impact. It supports the idea that social and individual behavior change will not happen because of isolated interventions but rather through the interaction of social, individual, and structural factors to produce an environment that supports behavior change. The SBC strategy’s conceptual framework explores potential outcomes at three distinct levels: policy, service delivery, and interpersonal.11
Through a consultative process, a detailed behavioral analysis identified and prioritized 23 critical behaviors for driving integrated early childhood development and ending violence against children in Oman. A cross-sectoral team (SBC TF) comprising officials from the Ministries of Health, Education, Information, and Social Development, as well as the National Center of Statistics and Information, governs the SBC strategy in Oman actively implemented the SBC action plan and adopted various social indicators to monitor and evaluate social change in Omani society.11
- Safe environments
To effectively mitigate child maltreatment and promote student safety within educational institutions, the Department of School in the MOH has executed a range of initiatives to enhance stakeholder collaboration across sectors and bolster the professional development of school nurses. School nurses provide training programs at schools and raise awareness among all stakeholders, including students, teachers, and parents, to ensure a safer environment for children. These programs have established a framework for school nurses to adhere to when addressing suspected cases of child maltreatment, consisting of two distinct routes: (a) they may refer the child to healthcare facilities for further intervention and take proactive measures by notifying the school director and completing a notification form at the school level, or (b) they may refer the case to the school director.12
School nurses receive training on protocols for adolescent health services, which include managing concerns such as accidental injuries and violence. This training program provides them with the necessary skills to evaluate and recognize health concerns related to adolescents in healthcare facilities and educational institutions. Additionally, it equips them with the necessary skills to conduct investigations, provide follow-up, and manage cases when identified risks arise.13 Collaboration between school nurses and social workers is essential to these measures for children’s wellbeing and safety.
- Parent and caregiver support
Despite general health education, Oman lacked formal parenting training until 2023, when UNICEF introduced behavior-informed training on early childhood development. The training emphasizes responsive feeding, positive discipline, and child development.14 This was followed by a collaborative training between the WHO and the Sultan Qaboos University Hospital to strengthen the training and ensure its inclusiveness.14,15 Positive parenting focal points are expected to spread parenting messages through one-on-one counseling sessions with parents at primary healthcare centers across Oman. This training is expected to expand and include teachers, community social workers, and other service-delivery personnel in the country.
The INSPIRE strategy emphasizes the importance of encouraging parents and caregivers to use positive, non-violent discipline, as well as engaging both parents and children in effective communication. This strategy advocates for the establishment of a social protection system, the implementation of parenting programs that educate parents about the importance of avoiding harsh forms of discipline, and the encouragement of countries to adopt home visitation strategies.5
Additionally, the Child Health Record (Pink Card), which is issued to each child born in Oman, was updated in 2024 to include positive parenting messages.
- Income and economic strengthening
The newly introduced Social Protection Law (Royal Decree 52/2023) was introduced to support at-risk individuals. The program provides financial support to all Omani children from birth until the age of 18 years. This initiative aims to enhance economic stability for families and reduce risks associated with child maltreatment.
- Response and support services
committees
The Child Protection System in Oman is state-sponsored. It has statutory functions directly provisioned by the MOSD, including heading the National Committee for Family Affairs, which is active in several areas related to child protection. Several committees are responsible for child protection matters and work at different levels for different functions, including high strategy and operational levels.16
the national committee for family Affairs
The National Committee for Family Affairs, established under the Royal Decree No. 12/2007, is a high-level committee with the mandate of formulating policies and strategies on family welfare. It is tasked with coordinating with official authorities and voluntary organizations and encouraging research in family matters. The committee oversees the work of the CPC and provides strategic directions when needed.
the central child protection committee
This is a high-level committee established within the MOSD under Ministerial Decree No. 65/2023. Its purpose is to formulate policies related to child protection and monitor their implementation. The committee directly supervises the work of the Regional Child Protection Committees in the governorates. It receives reports from these committees on child abuse cases that require a higher level of protection. The committee also recommends training activities for regional CPC members and conducts research on child protection.
the regional child protection committees (RCPC)
These are multi-disciplinary committees that act based on reports of any violence or violation of the child’s rights. They consist of members from various authorities, including the MOH, MOSD, Ministry of Education, Royal Oman Police, Public Prosecution, Sultan Qaboos University, Omani Women’s Associations, and two additional members who are selected by the Committee Chairman. They are available in the country’s 11 governorates and meet periodically to review cases and address case management challenges. The CPCs are critical for following up on cases and resolving issues relating to children’s safety, wellbeing, education, and support.16
hospital child protection committees (HSPC)
Hospitals mandate these multi-disciplinary teams to review suspected cases of child maltreatment, which they receive through direct admissions from the accident and emergency department, the CPC, or primary care centers within the governorate’s catchment area. To standardize their services, hospitals must establish HSPC teams and clinics under the direction of pediatricians who specialize in or have an interest in child maltreatment. HSPC teams perform medical evaluations of the identified cases in accordance with global standards. They receive reports of suspected cases from physicians from various hospital wards, including the emergency room. When such assessments are required, the evaluation team may request the assistance of an ophthalmologist and a radiologist. Additionally, the group comprises a social worker.8
The child’s history is obtained through interviewing the caregivers and, when possible, the child directly. When necessary, the HSPC team interviews other family members to corroborate the data. The team acknowledges the family’s perceptions and concerns, avoiding the common pitfalls of blaming the caregivers, and instead engages the caregivers in the management plan. Medical examination is conducted to check for signs of abuse or neglect and rule out other medical diagnoses. Where maltreatment is suspected, the MOSD ensures continuous liaison with the police, general prosecution, and the child protection delegate social worker assigned by the MOSD.
standardized operating procedures
Oman has implemented several strategies to improve its response to and support services for child protection, aiming to lessen the long-term effects of violence. To ensure the standardization of services across all levels of the health system and across different governorates in Oman, the MOH produced a number of standard operating procedures and guidelines to streamline the processes [Figure 3]. These include the national “Clinical Guidelines for Child Maltreatment and Neglect” and the national “Cross Sectoral Strategy for Coordination, Collaboration, and Referral of Child Maltreatment”.13
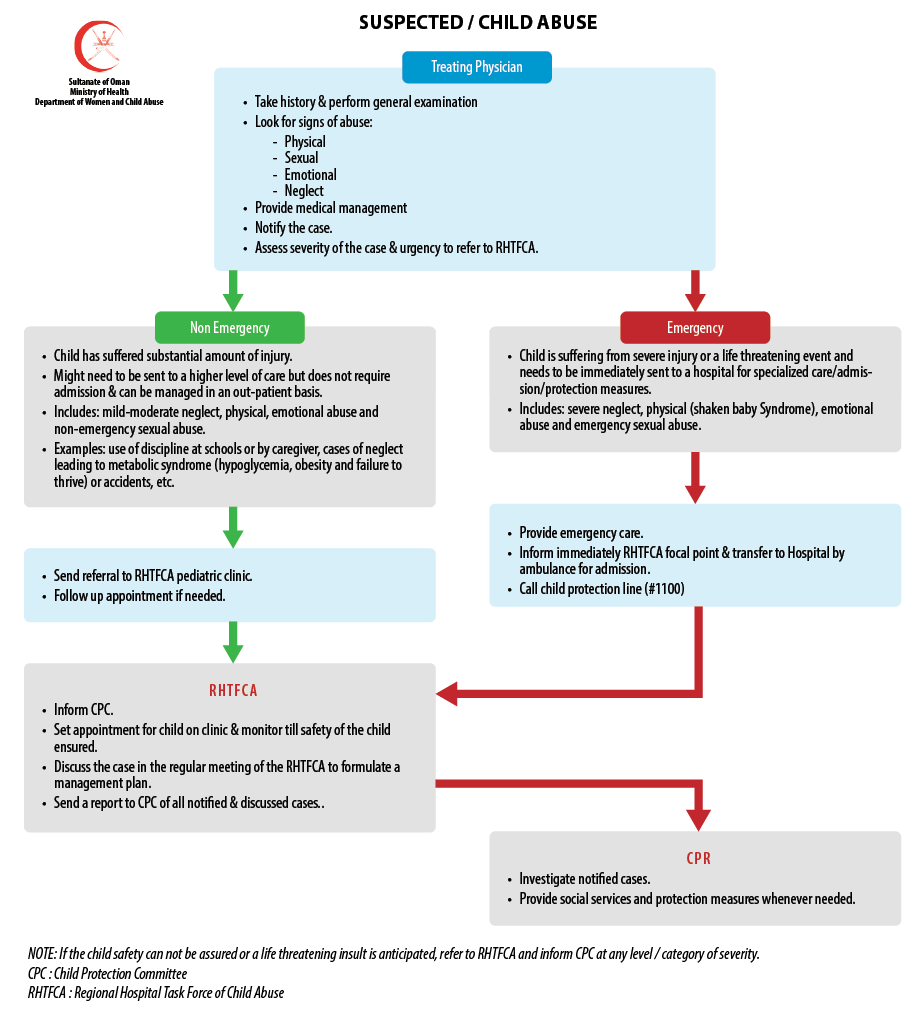 Figure 3: National Guidelines on case management of child maltreatment.
Figure 3: National Guidelines on case management of child maltreatment.
UNICEF and MOSD developed a national guideline on case management to standardize the reporting and management of child maltreatment across different sectors. It describes the roles and responsibilities of each sector, reporting on child maltreatment cases and their management across different sectors.
reporting of child protection
Two main sources of data on child maltreatment exist in Oman: the first is the national database of all cases reported by the community, schools, children themselves, and healthcare workers through the child helpline. The MOSD oversees this and considers it the official national source of information. The second is the reporting system by the MOH, which collects suspected cases of child maltreatment reaching health facilities. The MOH reviews reported cases for evaluation and referral as necessary. The CPC discusses all other cases at their periodic meetings and enters them into a database.15
- Education and life skills
Child maltreatment is now included in the curricula of medical students, nurses, and dentists at Sultan Qaboos University.15 The Oman Medical Specialty Board provides further on-the-job training in the residency programs of family medicine, pediatrics, and psychiatry. Additionally, each governorate conducts regular training on child maltreatment as part of the continuous professional development of healthcare professionals. Additionally, the introduction of specialized courses on “investigative interviewing” for child sexual abuse cases aims to improve the capacity of CPC members across sectors, including healthcare providers in MOH facilities. This includes training and capacity building in the child protection system and appropriate referral pathways, enhanced victim recognition, and underscores the significance of providing treatment, protection, and prevention services to children and their families.
Discussion
Governance, management, and enforcement form the foundations of child protection systems.17 Stakeholders have collaborated to initiate and implement several programs and services encompassing advocacy, governance, process streamlining, capacity building, data monitoring and evaluation, treatment, counseling, rehabilitation, and legal framework. These efforts have led to the fulfillment or partial fulfillment of the seven strategies listed in the INSPIRE strategy. However, due to the complexity of child protection and the required multi-sectoral services to deal with the cases, the real challenge remains coordinating efforts among different parties.8 The absence of an electronic case management system further exacerbates this issue, hindering case referrals and follow-ups. If left unaddressed, this gap may negatively impact case management and long-term outcomes.
We need to address the issue of centralizing interdisciplinary teams and rehabilitation services, as most psychologists, pediatricians, psychiatrists, and counselors are primarily accessible at the central level. Additionally, the lack of community-based services for children, including home-visiting nurses, further limits access to essential care and support.
Social norms and cultural attitudes also play a significant role in child protection challenges. In Oman, traditional perspectives on discipline, including the use of corporal punishment, remain prevalent.18,19 Addressing these norms requires sustained public education and parenting programs to gradually shift attitudes and promote positive parenting practices. Furthermore, healthcare professionals must be trained to recognize and respond to abusive behaviors and harmful parenting practices. The COVID-19 pandemic has introduced additional child protection concerns, particularly with increased online engagement among children and adolescents.20 Anecdotal evidence suggests a rise in cyberbullying, while the broader mental health impact of pandemic-related anxiety, uncertainty, and fear has been widely recognized. It is essential to implement measures that raise awareness among parents and caregivers about these risks. Additionally, children and adolescents should be educated on the positive use of social media, strategies for protecting themselves from cyberbullying, and avenues for seeking support when needed.
Lessons learnt and moving forward
This review highlights that Oman’s child protection system aligns with the INSPIRE framework; however, further improvements are needed, particularly in intersectoral coordination. Firstly, instead of focusing solely on responding to cases of child maltreatment, current efforts and strategies should shift their focus towards preventive measures, such as parenting programs. Numerous secondary preventive treatments have shown efficacy in other contexts. It is critical to continue creating and implementing community awareness and child maltreatment prevention programs, which are culturally appropriate, as well as social support programs to reduce the risks of depression in abused children.
Parenting programs could be one strategy to be implemented at three levels;
- Primary prevention
Targeting the general population with education on the risks of corporal punishment, the importance of communication, and the consequences of harmful disciplinary practices.
- Secondary prevention
Involving primary healthcare providers to support parents identified as having specific risk factors for child maltreatment.
- Tertiary prevention
Providing targeted interventions for parents who have been involved in incidents of child harm.21
We can integrate counseling on child protection and positive parenting as an integral part of the health services delivered to victims, thereby preventing many cases resulting from negligence or corporal punishment in the future.
At this stage, establishing an electronic case management system is crucial to enhancing referral and follow-up of cases among the different sectors and regions. All regions should complement this by ensuring adequate prevention, protection, and rehabilitation services at the community level.
Emerging problems such as bullying and cyberbullying, as well as the related mental health problems, necessitate immediate action to address their impact on children. There is a need to strengthen the CPC in both quantity and quality. A thorough assessment of their needs is necessary to understand the current gaps and how they can function more efficiently. Digitalizing the child protection system and improving stakeholder communication are necessary, increase the efficiency of the referral and follow-up system and enhance the integrity of available data. A case management system will support the coordination of services and integration with early childhood development programs.
The Ministries of Education, Health, and Social Development have endorsed the initiative and successfully piloted it in two governorates. We can better meet the diverse needs of vulnerable children and their families with a more effective and sustained impact by enhancing coordination between the respective sectors and existing services. The CMS will guarantee the identification of children in diverse settings such as schools and healthcare centers. We suggest establishing child protection centers across the various governorates in the future to facilitate the coordination of multidisciplinary service delivery.
Areas of future research
To inform policy and programming, population-based research on the incidence and patterns of child maltreatment in Oman is necessary. Standardizing data collection across sectors and governorates will enhance planning and intervention strategies. A comprehensive database on child maltreatment is essential for gaining a full understanding of the situation and guiding evidence-based decision-making.
Additionally, further research is needed to explore social norms and attitudes among parents, caregivers, and healthcare professionals regarding child maltreatment. Such findings will inform the design of interventions, including training programs on positive parenting and initiatives aimed at shifting harmful cultural practices.
Conclusion
Oman has implemented the strategies recommended by the INSPIRE program. However, there is a need for further improvement and coordination among relevant stakeholders. The urgent need for an electronic case management system to facilitate this coordination is evident. The country should prioritize the prevention of child maltreatment, including promoting positive parenting. This focus should be coupled with capacity-building for key professionals involved in childcare, including healthcare professionals.
Disclosure
The authors declare no conflict of interest. No funding was received for this study..
Acknowledgments
The authors acknowledge Dr. Shaima Darwish for her support.
references
- 1. Ministry of Social Development. Omani child law. 2014 [cited 2024 April 14]. Available from: https:// www.mosd.gov.om.
- 2. Weems CF, Russell JD, Herringa RJ, Carrion VG. Translating the neuroscience of adverse childhood experiences to inform policy and foster population-level resilience. Am Psychol 2021;76(2):188-202.
- 3. United Nations. United Nations Department of Economic and Social Affairs. Sustainable developmental goals. 2023 [cited 2024 January 20]. Available from: https://sdgs.un.org/goals.
- 4. World Health Organization. Ending violence against children through health systems strengthening and multisectoral approaches. 2022 [cited 2023 April 3]. Available from: https://apps.who.int/gb/ebwha/pdf_files/EB152/B152_21-en.pdf.
- 5. Social Determinants of Health. INSPIRE: seven strategies for ending violence against children. 2016 [cited 19 March 2023]. Available from: https://www.who.int/publications/i/item/9789241565356.
- 6. Koul R, Poothrikovil R, Al-Azri F, Al-Sadoon M. Evolution of epileptic encephalopathy in an infant with non-accidental head injury. Neurosciences (Riyadh) 2013 Jul;18(3):264-268.
- 7. Jackson AM, Kissoon N, Greene C. Aspects of abuse: recognizing and responding to child maltreatment. Curr Probl Pediatr Adolesc Health Care 2015 Mar;45(3):58-70.
- 8. Al Balushi SS, Morantz G, Dougherty G. The emergence of child protection capacities in Oman. Sultan Qaboos Univ Med J 2021 Nov;21(4):517-524.
- 9. UNICEF Oman. Charting progress towards child protection in Sultanate of Oman – findings of a national consultative workshop. Muscat, Oman: UNICEF 2009. p.6.
- 10. World Health Organization. World report on violence and health. 2002 [cited 2023 March 19]. Available from: https://www.who.int/publications/i/item/9241545615.
- 11. UNICEF. UNICEF Oman in 2023 achievement and key results. 2024 [cited 2024 January 5]. Available from: https://www.unicef.org/oman/reports/unicef-oman-annual-report-2023.
- 12. Haas JJ. The role of the school nurse in detecting and preventing child abuse during this age of online education. NASN Sch Nurse 2021 Jan;36(1):16-19.
- 13. UNICEF. Situational analysis of children and women in Oman 2017. 2017 [cited 2024 January 14]. Available from: https://www.unicef.org/oman/reports/situational-analysis-children-and-women-sultanate-oman-2017.
- 14. Al-Mahrooqi R, Denman C, Al-Maamari W. Omani parents’ involvement in their children’s English education. SAGE Open 2016 Jan;6(1):2158244016629190.
- 15. Al-Mamari W, Idris AB, Al-Alawi K, Rashid N, Al-Araimi FA, Siddeeg K. Enhancing child development in Oman: applying global agenda into local context. Sultan Qaboos Univ Med J 2023 May;23(2):143-147.
- 16. Al Abduwani JA. Assessing the reliability and validity of the child abuse potential inventory in Arabic language among pregnant women in Oman. 2018 [cited 2024 February 15]. Available from: https://wrap.warwick.ac.uk/id/eprint/117705/.
- 17. Bruning MR, Doek JE. Characteristics of an effective child protection system in the European and international contexts. Int J Child Maltreat 2021;4(3):231-256.
- 18. Al Abduwani JA, Ahmed MK, Barlow J. Assessing the reliability and acceptability of an arabic version of the child abuse potential inventory. Child Abuse Rev 12 Nov 2020;29(5):477-492.
- 19. Taylor CA, Hamvas L, Rice J, Newman DL, DeJong W. Perceived social norms, expectations, and attitudes toward corporal punishment among an urban community sample of parents. J Urban Health 2011 Apr;88(2):254-269.
- 20. Al Jadidi S, Al Harrasi M. The psychological impact of covid 19 pandemic on the general population of Oman: a national community based study. Mal J Med Health Sci 2022 Sep;18(5):114-121.
- 21. Carroll P. Effectiveness of positive discipline parenting program on parenting style and child adaptive behavior. Child Psychiatry Hum Dev 2022 Dec;53(6):1349-1358.